Juniper Publishers Cancer Therapy & Oncology International Journal is dedicated to publish the contributions on all aspects of experimental and clinical cancer research. CTOIJ is a multidisciplinary, Open Access, peer reviewed journal accepts Research, Review Articles, Short Communications, Mini- Review, Case Reports, Opinions, Letter to Editors etc
Multiple Metastatic Small Cell Carcinoma of Unknown Primary Diagnosed on Inguinal Node Biopsy- Juniper Publishers
Get link
Facebook
X
Pinterest
Email
Other Apps
Cancer Therapy and Oncology — Juniper Publishers
Abstract
Poorly differentiated neuroendocrine tumors are uncommon neoplasms of the lung and the gastrointestinal tract. However, 3–5% of these tumors are diagnosed as metastatic disease with unknown primary. Here, we describe a case of neuroendocrine small cell carcinoma of unknown primary diagnosed by inguinal node biopsy. A 53-year-old male patient with a history of heavy smoking presented with cough, back pain and altered mental status. Whole body imaging studies (CT — MRI — FDG PET) favored a diagnosis of hematological disease (lymphoma) or diffuse metastatic melanoma. However, inguinal node biopsy revealed morphological and immunohistochemical features of a neuroendocrine carcinoma, probably originating from the lung. The patient received palliative whole brain irradiation and etoposide/platinum-based chemotherapy.
Abbreviations: CUP: Cancer of Unknown Primary; IHC: Immunohistochemistry; CT: Computed Tomography; MRI: Magnetic Resonance Imaging; PET: Positron Emission Tomography
Metastatic cancer of unknown primary (CUP) accounts for 3–5% of all malignant neoplasms. International registries from seven countries have reported incidences ranging from 2.3% to 7.8% [1]. More than 50% of CUP patients present with multiple sites of involvement, while the rest have a single site. The progression of such cancer with unknown origin is rapid in most cases and shows atypical metastatic patterns. Most frequent locations of dominant metastatic sites are mediastinum, retroperitoneum and peripheral lymph nodes [2]. CUP is also more common in lymph nodes of the neck and axillary regions, while inguinal involvement accounts for <5% of cases [3]. Since CUP in the inguinal region is rare, there is a paucity of literature on the management of such patients.
Neuroendocrine carcinomas with widely varying clinical and histologic features account for approximately 3% of all CUP [4]. Neuroendocrine cells are distributed widely throughout the body and neoplasms of these dispersed cells can occur at many sites. Of major importance is the classification of this group into tumors with low-grade histology (classic carcinoid) and indolent clinical course vs those with high-grade histology (small or large cell with neuroendocrine features) and an aggressive clinical course [5]. The origin of these high-grade neuroendocrine carcinomas remains unclear. Panels of immunohistochemical (IHC) stains or molecular gene expression tumor profiling are used for the determination of the tissue of origin in CUP patients [6]. CUP of the neuroendocrine type may have arisen from an occult extra-pulmonary site, but are correctly described as neuroendocrine car¬cinoma of an unknown primary site. Patients with small cell carcinoma at a metastatic site are considered for systemic therapy at the time of diagnosis. Although the optimum regimen is undefined, a platinum/etoposide-based regimen is currently used [7]. In this case report, we describe an uncommon case of inguinal lymph node small cell metastasis of unknown origin, accompanied by multiple sites of involvement.
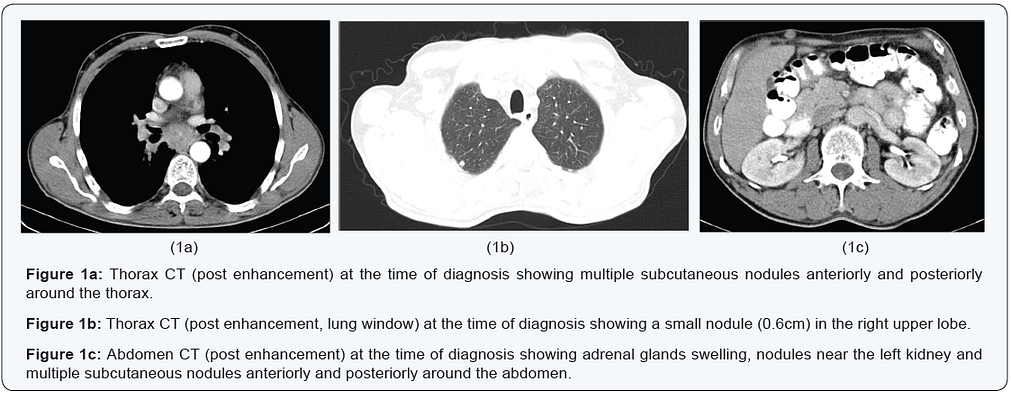
A 53-year-old male, with a history of heavy smoking, presented with polyuria, polydipsia and episodes of transient memory loss. He suffered from back pain, night cough, cyanosis and an altered mental status. There was no history of fever or night sweats. On clinical examination, there were multiple palpable subcutaneous nodules on the trunk and tenderly swollen inguinal lymph nodes. The remainder of clinical examination and initial laboratory investigations had normal findings. The results of laboratory examinations, including urinalysis, liver and renal function tests, revealed no abnormalities. Upper and lower gastrointestinal endoscopy was normal. Serum carcinoembryonic antigen, carbohydrate antigen 19–9 and prostate specific antigen were within normal range. Cytology examination of the sputum was negative. The contrast-enhanced computed tomography (CT) scan of the chest revealed emphysematous blebs/bullae, enlarged mediastinal lymph nodes and a suspicious (6mm) nodule in the upper lobe of the right lung. The CT scan of the upper and lower abdomen revealed adrenal glands swelling, nodules near the left kidney, multiple subcutaneous nodules anteriorly and posteriorly around the thorax and the abdomen as well as enlarged inguinal lymph nodes (Figure 1).
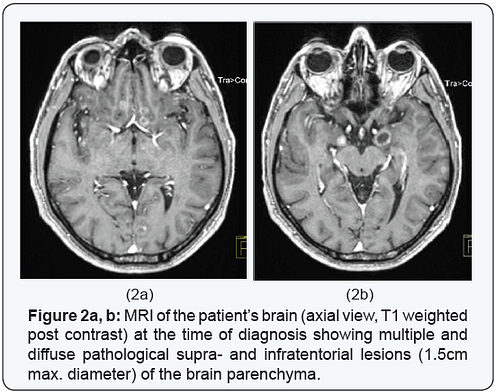
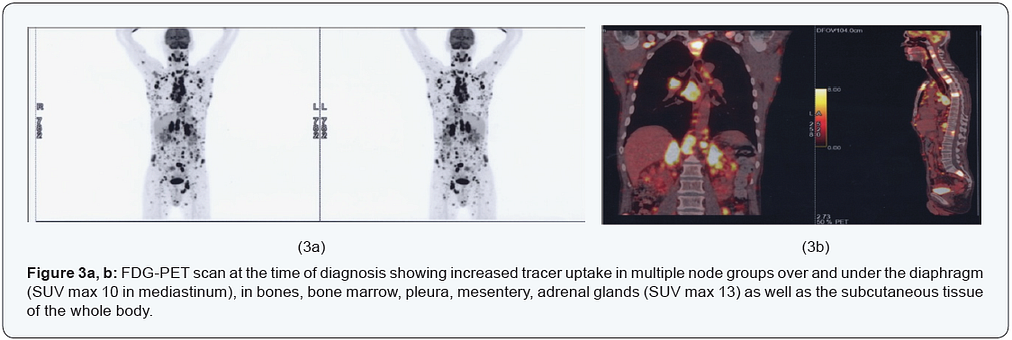
Magnetic resonance imaging (MRI) of the brain revealed multiple and diffuse pathological supra- and infratentorial lesions (1.5cm max. diameter) of the brain parenchyma (Figure 2). With no primary site of cancer identified, the patient underwent an excisional biopsy of a left inguinal lymph node. Histopathology was suggestive of small cell carcinoma probably originating from the lung. The IHC stains for TTF1, CK7 and synaptophysin were positive and also revealed high expression of Ki-67 (>80%). In order to find the primary lesion diagnosed by biopsy of the inguinal lymph node, a positron emission tomography (PET) scan was performed. This showed increased tracer uptake in multiple node groups over and under the diaphragm (SUVmax 10 in mediastinum), in bones, bone marrow, pleura, mesentery, adrenal glands (SUV max 13) as well as the subcutaneous tissue of the whole body (Figure 3).
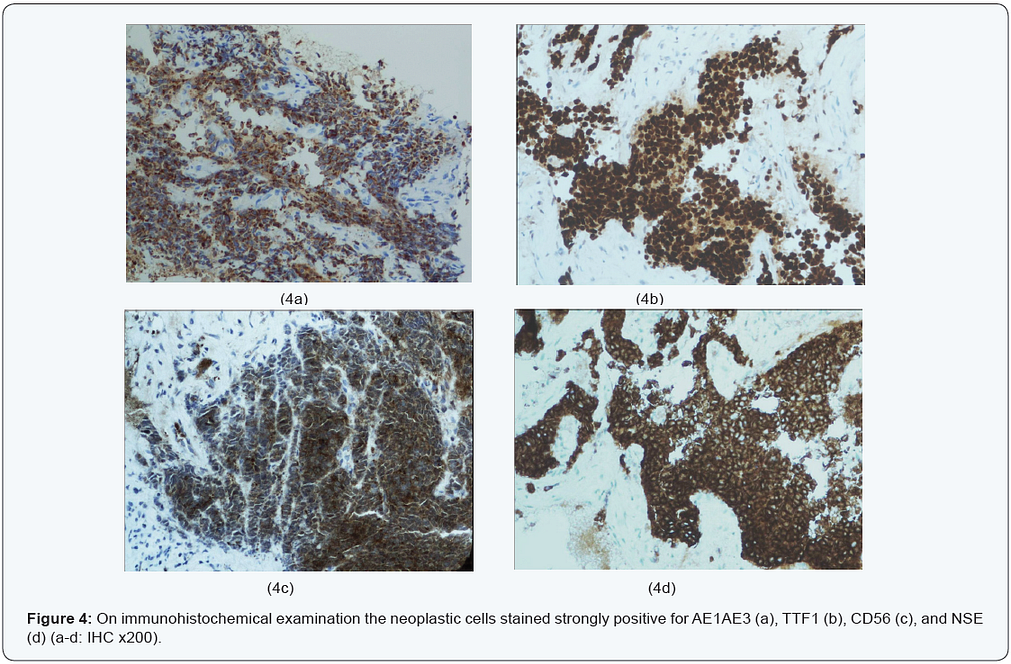
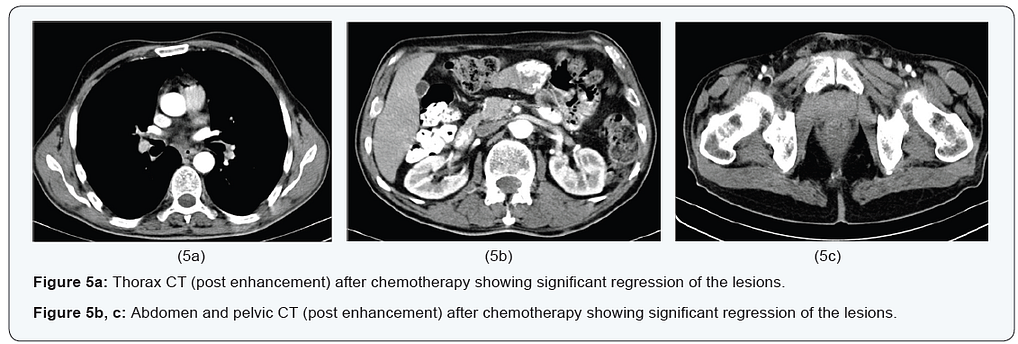
Lungs, liver, spleen and pancreas revealed no tracer uptake. The primary site could not be visualized generating a differential diagnosis between hematological disease (lymphoma) and diffuse metastatic melanoma. Finally, the histopathological diagnosis was reviewed and confirmed by the pathologists of our Hospital. An appropriate battery of immunostains revealed the following immunophenotype: AE1/AE3+, CK8/18+, TTF1+, CD56+, NSE+, synaptophysin++/-, chromogranin — /+, CK7 — /+, CK20-, CD45-, S100-, NF-. Cell proliferation index Ki67/MIB1 was high (>80%). The lymph node metastasis showed morphological and immunohistochemical features of neuroendocrine small cell carcinoma (Figure 4) indicating a possible primary site in the lung. Palliative whole brain radiotherapy was performed in our department delivering 30 Gy in 10 fractions. Significant clinical improvement in terms of memory loss was immediately observed. Chemotherapy was administered as a platinum/ etoposide-based combination schedule with remarkable clinical response immediately. After chemotherapy, the CT imaging study confirmed substantial regression of all metastatic lesions (Figure 5).
Our patient suffered from cough, worsening back pain and altered mental status. He clinically presented multiple palpable subcutaneous nodules on the trunk and swelling of the groin lymph nodes. At FDG PET, the lungs, the liver, the spleen and the pancreas revealed no tracer uptake raising the suspicion of hematological disease (lymphoma) or diffuse metastatic melanoma. However, the diagnosis of neuroendocrine small cell carcinoma was established by the characteristic morphology on histology and an IHC neuroendocrine marker pattern (CD56, chromogranin, synaptophysin, TTF1). Patients with small or large cell histology and a history of cigarette smoking should be suspected of having an occult lung primary. Our patient presented widespread metastatic disease, for which no primary site could be detected after clinical examination and extensive investigations.
CT scan revealed no mass lesions, except a small indeterminate nodule in the lung. It is rather unlikely for this to have been the primary site as the nodule was very small and negative on PET-CT. CUP is a diagnosis of exclusion, since many studies did not include other types of tumors such as lymphoma, melanoma and sarcoma, as well as tumors of unusual primary sites. However, since those types of carcinomas often enter the clinical and pathological differential diagnosis, they should be considered [5,8]. The diagnostic procedure begins, if necessary, by determining the cell lineage (epithelial, melanocytic, lymphoid, mesenchymal or germinal) with the aid of appropriate IHC markers. The choice of the IHC panel deeply influences subsequent diagnosis. In some cases IHC algorithms can allow the identification of a primary site with adequate accuracy [9].
Metastases of unknown primary origin are divided in two groups: 1) those in which the primary site might be defined at least by their IHC profile; 2) those which really remain ‘orphan’ even after an appropriate IHC screening [10]. The primary site may either have a slow growth or may possibly become involute and therefore unlikely to manifest itself. In some instances, although the metastatic pattern is often unpredictable, the site of primary origin can be found during lifetime or autopsy. Generally it is a small nodule often localized in the lungs or in the bilio-pancreatic tract [11]. Since the unknown primary mass can be located anywhere in the body, a cross-sectional whole-body imaging modality is the proper method to search for it. Small lesions or pathological changes in normal-sized tissues can be missed by CT and MRI [12]. From this perspective, PET using the radiotracer 18 F-fluoro-2-deoxyglucose is the leading approach, since it provides functional and metabolic information.
Notably, PET/CT imaging is known to have good sensitivity and specificity, mainly in head/neck and lung cancers [13]. Patients with high-grade neuroendocrine tumors are initially responsive to combination chemotherapy and should be considered for a trial of treatment. However, the treatment is approached similarly to extensive stage small cell lung cancer, as these cancers have similar histology. Treatment includes standard chemotherapy used to treat lung cancers, including platinum-based or platinum-taxane combination chemotherapy. This group of patients presented response rates up to 55% with 20% complete responders and overall survival of 15 months as well as almost 10–15% long-term survivors [14].
Cancer Therapy & Oncology- Juniper Publishers Abstract Popularized as the “Sister Joseph’s nodule” is the metastatic lesion of the umbilicus. Hitherto, cases had been reported worldwide. Therefore, this article aims to document the patterns of it obtained among an ethnic group in a developing community. Incidentally, a few indigenous doctors suspected the lesions to be of the Sister Joseph nodule type. The epidemiological data included equality of sex and the preponderance of adenocarcinomas. Keywords: Carcinoma; Umbilicus; Metastasis; Age; Type; Sister Joseph Nodule Introduction Metastatic carcinoma of the umbilicus gained prominence when, “during the early days of the Mayo Clinic, Sister Mary Joseph, the superintendent of St. Mary’s Hospital and Dr. William Mayo’s frequent first assistant, ...
Cancer Therapy & Oncology - Juniper Publishers Abstract This article aims to standardize terms used in Surgical Oncology that are the basis for the treatment of cancer patients. Terms like: Patient out of cancer treatment, Patient in stage IV, In block tumor resection, Ganglionic relay, Local and regional control, Systemic Control, Unknown Primary Origin, Unresectability, Inoperability, Multiple Organ Resection, Preoperative Nutritional Status, Minimum Oncologic Procedure, Resection margins, Prognostic Factors, Peritoneal Washing Cytology, Adjuvant, Neoadjuvant and Peri-adjuvant Therapy. Keywords: Basic terms in Surgical Oncology; Cancer Surgery Abbreviations: OCT: Patient Out of Cancer Treatment; UPO: Unknown Primary Origin; BMI: Body Mass Index. Introduction There are basic oncological principles universally accepted and those principles were born from the experience accumulated in Cancer Treatment Centers after years of observing the results ...
Cancer Therapy & Oncology- Juniper Publishers Abstract A Birmingham (UK) group considered in 1980 that the establishment of a Histopathology data pool encourages epidemiologic analysis. Consequently, the senior author (WIBO) had such an advantageous opportunity. Interestingly, the junior author (GEN), working in a near Surgical Outpatient Clinic, was consulted by a gravid 5, para 8, patient, i.e., one twin and a set of triplets. Moreover, she also developed 3 breast carcinomas. Therefore, this paper is documented in order to stimulate worldwide interest in this peculiar combination. Is it only happenstance or an explicable natural event?. Keywords: Breast, triple cancer, pregnancy, triplets, Igbos, epidemiology Introduction The breast has for centuries been the medical man’s talking po...









Comments
Post a Comment